Hospitals Need a ‘No-Fragrance’ Rule
My 85-year-old mother recently had to go to the hospital emergency room for a subdural hematoma. She’s very sensitive to fragrances. Members of her bridge club and singing group know this and respect her wish for no fragrances. Otherwise her eyes and nose water, she gets headaches and has difficulty breathing.
 |
|
Hospitals need to enforce rules because fragrances can aggravate the conditions of patients. Photo: U.S. Navy. |
At the ER, a nurse who was very friendly smelled so strongly that I asked him not to come close. It was the beginning of the shift. He apologized and washed it off, thankfully, but he needed to hear this from a patient’s mother who is also a doctor! I do plan to contact the director of nursing services.
People who are pregnant, get migraines or other headaches, or have asthma often need to avoid fragrances. Many hospital staff members themselves are very sensitive because they have been previously TILTed.
- Related Post: How to Thank People Who Wear No Fragrances
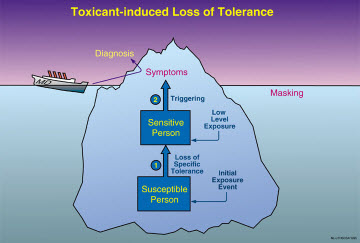
TILT is short for Toxicant-induced Loss of Tolerance. It affects people who have repeated low-level exposures, such as in a “sick building,” or a one-time, high-level exposure such as a chemical spill or pesticide application. TILT can cause chemical intolerances that impair a person’s health, ability to work or go to school, and other everyday activities. There’s a widely accepted screening instrument to help identify TILT, called the QEESI, or Quick Environmental Exposure and Sensitivity Inventory. It’s free to download.
Hospital staff members need to avoid wearing fragrances. This is important because patients may be unable to speak for themselves. Even worse, fragrances may precipitate vomiting in chemotherapy patients whose treatments cause nausea. And there’s certainly a need for a no-fragrance rule around newborns, babies or children, and in the intensive-care or critical-care units.
Fragrance policies for the health-care industry are emerging. Some examples:
- The Centers for Disease Control has issued a policy governing its installations.
- A Canadian organization, Bryant Community Healthcare System, for example, applies a policy for both employees and patients.
- And the Massachusetts Nursing Association published an excellent article as far back as 2006 explaining the value and way of setting up such a policy.
I don’t recall fragrances being such a problem when I was a medical student in the 1980s. Then it was tobacco smoke — first hand, second hand and third hand — and smoke retained in patients’ clothing and on their breath. We medical students would stand as far away as possible from these patients when we told them to take a deep breath and exhale. Now people come in the hospital and leave “vapor trails” of fragrances behind them — in elevators, corridors and stairwells.
Fortunately for my mother, I’m a professor and assistant dean for the dual degree MD/MPH program at the UT School of Medicine, which is directly across the street from the hospital. I’ve published many papers, books, and a screening questionnaire for assessing chemical intolerance, but not everyone knows this.
Before I left her bedside last night, she asked for a stack of my business cards so she could pass them around.