The Pulitzer Prize-winning publication ProPublica drew attention in May to the lack of centralized data on implanted medical devices. Where can patients find out when a pacemaker, breast implant or artificial hip, for example, goes bad?
Not from the U.S. Food and Drug Administration, as ProPublica’s story describes. Prescription drugs have unique codes the government can use to track problems. But implanted devices? No such luck.
And there’s an unexplored dimension to the implant question: Implants are “xenobiotics,” petrochemical products that pose particular concern for people who may be more chemically susceptible.
I testified before the FDA in 2005 about the dangers of implants, and cited evidence from my own research.
Over a decade ago, in 1999, along with co-author Thomas J. Prihoda, PhD, I reported on a group of patients who received implants and subsequently developed chronic health problems and chemical intolerances that they had never experienced before.
Although inserting implants certainly differs from inhaled exposures to pesticides or air contaminants in a sick building, for susceptible individuals it seems like the body doesn’t care whether the exposure is exogenous (like air pollutants) or endogenous, like an implant. The consequences can be similar — chronic, multi-system symptoms and intolerances for foods, alcoholic beverages, caffeine, everyday chemicals like cleaning agents, engine exhaust, fragrances, and even medications like antibiotics or antidepressants. Once people become ill, not just the implants, but everyday exposures like these can trigger symptoms and perpetuate illness.
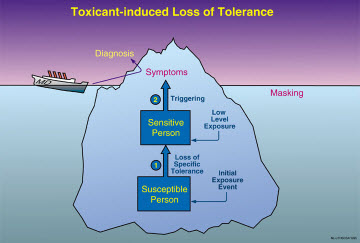
We obtained exposure histories from patients who became ill following an “exposure event” — ill veterans from the first Gulf War in Iraq, people exposed to pesticides or remodeling chemicals, and patients who had received an implanted medical device. The groups shared illnesses marked by multiple symptoms and new intolerances — the hallmark symptom of the illness process Toxicant-induced Loss of Tolerance (TILT).
Patients with implants reported symptoms affecting multiple organ systems which frequently involved cognitive and mood difficulties.
The implant group included 87 individuals, 97 percent women, mean age of 50. Most had received breast implants or temporomandibular joint (TMJ or jaw) implants. Two-thirds said their device had ruptured. Nearly all of those reporting difficulties said their illnesses had affected their ability to work. Their most pervasive symptoms involved muscle and joint problems.
TILT is often overlooked in implant patients when doctors don’t recognize it. There is a saying in medicine: You can’t make the diagnosis you don’t think of. And many doctors don’t know that multiple symptoms and intolerances point to TILT. In medical school, we are often taught that the more symptoms a patient reports, the less likely there is anything to them — in other words, the problem is psychogenic. While many patients suffer from psychological symptoms such as depression, anxiety and cognitive difficulties, even confusion, it is important to remember that psychological symptoms are not necessarily psychogenic. Many physical illnesses can cause similar symptoms, for example, autoimmune diseases, multiple sclerosis and Lou Gehrig’s disease (ALS).
As I wrote in the 1999 study, “The fact patients reported such diverse symptoms led some physicians to conclude that none of them rises to the level of a medically identifiable syndrome. Nor are these conditions explained by current, generally accepted mechanisms for disease.”
I developed the QEESI, or Quick Environmental Exposure and Sensitivity Inventory, several years ago to help doctors and patients make sense of multiple symptoms and measure the potential for chemical intolerance.
Persons who score high on the QEESI, a validated and published screening instrument, may be at greater risk if they receive an implant or have other exposures, e.g., anesthetics, drugs, pesticides, remodeling of their home or workplace, etc. To determine whether you may be at increased risk of developing TILT, you can take the QEESI to gauge your own susceptibility or to document changes in your symptoms and intolerances as a consequence of an implant or its removal. Many individuals do report improvement in symptoms once their implants are removed.
As for the FDA, the regulatory agency has done poorly in its role of gathering scientific data about the safety of implants. Dr. Diana Zuckerman, president of the National Research Center for Women and Families, a research and education group, told an expert panel of the FDA in 2011 that some breast implant manufacturers had failed to carry out the FDA’s own recommended studies of post-implant patients. One of the FDA’s chief scientists, Dr. William Maisel, later acknowledged shortcomings when questioned by the New York Times.
Commenting on breast implants in her blog, Dr. Zuckerman added, “Silicone implants are considered biocompatible, which means that most patients won’t have an allergic or autoimmune response. But, that doesn’t mean that nobody will. In fact, the implant companies intentionally excluded women with autoimmune histories from their studies because of concern that the women would have medical complications that would jeopardize getting FDA approval.”
When I’ve testified before the FDA on the results of our study, I’ve been concerned with the fact that parents may purchase implants for their daughters for their “Sweet 16” or high school graduation. Adverse events include scarring as well as chemical intolerances in a subset of individuals. The problem is, that before an implant, there is currently no way of knowing who may be more susceptible to developing health problems or disfigurement. The QEESI might at least make women more aware if they are susceptible to petrochemical exposures, including implants. I’ve heard of women who already had been diagnosed with an autoimmune disease going to see a doctor to get implants. No doctor should agree to place breasts implants in women with this history.
Also, I’m aware of young women borrowing money to get an implant. However, if they become ill, insurers may not pay to have them removed. So it’s not just the cost of the implant, but the unplanned costs if removal becomes necessary.