|
|
Guest blogger Laura MacCleery describes her do-it-yourself room painting project and things you should know before painting a room. Laura is a lawyer, mother and self-described “squeaky wheel in search of a spoke.” She writes commentary at Laura’s Rules. Her post first appeared there on Feb. 1.
|
By Laura MacCleery
What to do with a low-ceilinged, windowless basement room? Give it to the toddler, of course …
But then, it just screams for some cheer. When my friend Lisa showed me the charming mural she had painted on her son’s wall in honor of his adoption, it was inspiring. She told me how she made the cute and life-like clouds using nothing more than a sea sponge and some water-based tempera paint.
I could do that, I thought. So sometime in my feverish, flu-like state, after days of uselessly prowling the house over the holidays, I determined to accomplish some little thing, at least.
The most manageable (and thoughtless) project on my list was introducing a little whimsy to the “playroom.” It mainly functions as a toy storage area these days, given Maya’s inability to be in the basement by her lonesome. But I have hopes, my friends, that someday she will be capable of independent play, and so this is for that day.
First, because it’s me and this blog and all, I must point out what you know already: paint is notoriously toxic. This is a particular concern in a poorly ventilated basement. As the wonderful Diane MacEachern of Big Green Purse (another Takoma Park green blogger!), writes:
Conventional paint contains many volatile organic compounds, or VOCs, that “outgas” and escape into the air after they are applied. Indoors, these VOCs cause headaches, nausea, achy bones, and general discomfort. Outdoors, they contribute to smog and air pollution.
And they smell nasty, which can’t be good. The VOCs include chemicals like terpenes, formaldehyde, acrolein, phthalates, glycol, toluene, methylene chloride, styrene, trichloroethylene, xylenes, and benzene, among others. Any one of these is enough to make me gag, personally. A terrific new guide to building a non-toxic nursery, out just today from our friends at Healthy Child, Healthy World, provides very helpful information about paint types suitable for a nursery or other rooms on p. 16 of their new, interactive ebook and less toxic options. They also have 7 helpful tips for healthier painting. Basically, the best way to go is real zero-VOC paints (i.e., ones that completely and verifiably lack toxics or solvents), or with natural, organic or milk-based paints.
Our local hardware store only stocks the zero-VOC kind, but they at least have a really good brand — Mythic, which I have used on several rooms in our house with excellent results. Mythic is a “real” zero-VOC paint, with no toxics like lead or other known toxins in it, and is also solvent free and it goes on beautifully.
In fact, it’s so clean, it doesn’t need a warning label like most paints. (Lullaby Paints appears to be another great option, but I have not used them myself.) Even using Mythic, I set up a fan to speed the paint drying process, open a window when possible, and do not use the room for at least several days.
Before painting, you should also be aware that many, if not most, paints labeled “zero-VOC” can be problematic, because the colorants still contain VOCs and once they are added, then the paint is “zero-VOC” no longer.
In fact, the Federal Trade Commission just sued Sherwin Williams over false claims on this issue, and won, sort of. The companies now at least have to say, somewhere, that the zero-VOC claim applies only to the base paint and that the VOC levels can be impacted by the dyes. From The Consumerist:
In truth and in fact, in numerous instances, Pure Performance paints do not contain zero VOCs after color is added,” alleged the FTC.
To settle these claims by the agency, both paint companies are prohibited from claiming their paints contain “zero VOCs,” unless, after tinting, they have a VOC level of zero grams per liter.
The companies can continue claiming “zero VOC” if they “clearly and prominently disclose” that the “zero VOC” statement applies only
to the base paint, and that depending on the consumer’s color choice, the VOC level may rise.
At any rate, back to the fun part. For the playroom, I first painted one wall and a strip of a wall in a bright, sunny yellow. One coat was enough to do it. Then, I covered the ceiling in a light blue paint left over from a sample I considered using for Maya’s upstairs room (Ocean Falls was the color). (Yes, her bedroom is blue. And lovely.)
I didn’t bother taping for the ceiling, as the indistinct edges add to the effect. Mythic is also forgiving; a wet sponge used soon after painting will clean up any messes.
Then, using the sea sponge and a pool of paint in the pan, I painted swirls in large circles across the ceiling with a slightly darker blue, called Peace River.
Last, I added white clouds around the lights and all over the ceiling in various sizes using the sponge dipped in Crayola white tempera paint. This can also be easily fixed with a wet sponge while the paint remains wet. I tried to leave a little extra paint in some places for a slight texture.
I was pleased with the result, which adds a dreamy quality to a small, boxy room. And Maya likes it too!
|
|
|
|
Tags:
Big Green purse,
Business,
ceiling,
chemicals,
Child,
children,
clouds,
Consumerist,
Crayola,
decor,
decorations,
DIY,
easy,
eco-,
environmental health,
Family,
Federal Trade Commission,
green,
health,
healthy,
Healthy Child,
Healthy World,
Home,
infancy,
Infant,
infants,
low-VOC,
Lullaby,
mommy blog,
mythic,
Nature,
nursery,
organic,
Paint,
Parent,
parenting,
parents,
playroom,
safety,
sea sponge,
Sherwin Williams,
simple,
sky,
sponge painting,
toddler,
tots,
Toxic,
toxic chemicals,
toxics,
voc,
Volatile organic compound,
wall,
zero-VOC Category:
Health |
Comment
December 19, 2012, 6:09 pm
The Japanese cedar was never known to cause allergic rhinitis in Japan until the 1960s even though the tree had been indigenous to Japan for more than a million years. Recognition of cedar-induced rhinitis and an increase in cases in Japan coincided with lenient regulation of diesel exhaust and increased numbers of diesel vehicles in that country.
What does cedar (really a juniper) allergy have to do with diesel exhaust? Exposure to petrochemicals such diesel exhaust, can lower a person’s tolerance for “natural” substances such as pollen, mold, dust mites and animal dander, leading to allergic reactions. Researchers in Japan have confirmed that exposing mice to diesel exhaust increases their IgE production, the immunoglobulin associated with allergy.
What does this have to do with TILT, or Toxicant-induced Loss of Tolerance? People who become chemically intolerant, or TILTed, frequently report amplified allergic responses. This relationship may help explain the rise in allergic rhinitis in Japan. It explains why the QEESI, or Quick Environmental Exposure and Sensitivity Inventory, asks about a person’s exposures to diesel exhaust and any associated heightened allergic responses.
I know how potent cedar pollen can be. I live in Central Texas, on the edge of the scenic Texas Hill Country. Despite its beauty, the Hill Country has hundreds of thousands of Texas Mountain Cedars that shed notoriously allergenic pollen. From December to February, the pollen causes such severe symptoms that sufferers call it “cedar fever.”
Tags:
allergen,
allergies,
cedar,
cedar fever,
diesel exhaust,
Hill Country,
IgE,
immunoglobulin,
juniper,
pollen,
QEESI,
Quick Environmental Exposure and Sensitivity Inventory,
rhinitis,
Texas,
tilt,
toxicant-induced loss of tolerance Category:
Health |
Comment
December 14, 2012, 7:33 pm
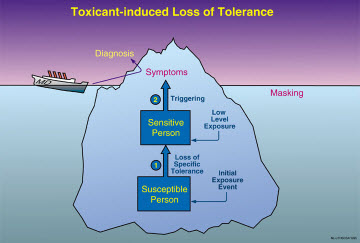
The shooting tragedy at Sandy Hook Elementary School in Newtown, Conn., underscores the urgency for mental health practitioners to understand the TILT iceberg. The iceberg is a graphical depiction of the risks for people with Toxicant-induced Loss of Tolerance.
Practitioners need to take a proper history of their patients and think about the role of petrochemicals/drug exposures in violence. These hair-trigger anger reactions were not uncommon among chemically-exposed Gulf War veterans I saw as a consultant for the Veterans Administration. The veterans had become chemically intolerant and were so afraid they might harm their own families that they gave their guns to friends for safe-keeping.
Dietary intolerances are one of the main consequences of TILT, based upon our extensive studies of people who became ill following exposure to pesticides, solvents, substances used in remodeling, and Gulf War chemicals.
Prisons are controlled environments in which it’s been shown that reducing exposures, even to such benign chemical substances as sugar, can reduce violence.
Read an in-depth exploration in the book I co-authored,
Chemical Exposures: Low Levels and High Stakes.
The Sandy Hook shootings, like those earlier in Oregon, Colorado and elsewhere, appear random but individuals whose limbic systems have been sensitized by exposures and then are triggered by cleaning agents, foods or medications they no longer can tolerate are more likely to pick up a gun and use it.
Using the QEESI, or Quick Environmental Exposure and Sensitivity Inventory, with patients and reducing exposures (pesticides, solvents, etc.) could help. TILT may be responsible for a small subset or a large number of cases, but almost no mental health professionals are aware of this illness dynamic/new paradigm and they must not miss the diagnosis. Too many lives are at stake.
Tags:
cause,
chemical exposure,
Chemical intolerance,
Connecticut,
environmental,
food intolerance,
Gulf War,
guns,
mental health,
mental instability,
Newtown,
psychiatrists,
psychologists,
QEESI,
Sandy Hook,
shootings,
social workers,
tilt,
violence,
weapons Category:
Health |
Comment
December 5, 2012, 6:48 pm
|
|
Describing preparations for Hurricane Sandy, guest blogger Laura MacCleery gives a humorous example of the old adage about how “no good deed goes unpunished.” Laura is a lawyer, mother and self-described “squeaky wheel in search of a spoke.” She writes commentary at Laura’s Rules.
|
By Laura MacCleery
When I recently filled out a helpful questionnaire on chemical intolerance, the Quick Environmental Exposure and Sensitivity Inventory (QEESI), or “Queasy” as I like to call it among friends, a screw-shaped light bulb went off. (Compact fluorescent, of course.)
According to the results of this scientifically validated tool for measuring sensitivities to toxins in our environment, I am on the “high” end for both exposures and symptoms, meaning that I don’t tolerate smells like gasoline and off-gassing furniture well.
The survey powerfully showed why I obsess about such things, while other people may shrug them off. Seeing how I scored was important to me because it identified some common sources for the headaches and other discomfort I often experience following exposure to an unpleasant chemical-laden odor.
Most of the things on the list on the QEESI, which is a quick inventory, as the name implies, including bleach-based cleaning supplies or a “new car” smell, can make me feel a bit off, even in small doses. I still remember being newly pregnant in a Washington, D.C., wintertime and driving with the windows way down, the cold wind in my face, because freezing was far preferable to the vinyl smell emanating from my brand-new Nissan, especially given my bionic nose from the pregnancy!
But that sensitivity hasn’t gone away since I had my daughter, either. And I’m not the only one who’s bothered by the fragrances crowding our environment. A recent article in a UK newspaper notes that: “One leading expert suggests nearly a third of people suffer adverse health effects from being exposed to scents.”
The article explains:
“Allergies are on the increase, and the amount of perfumed products is also on the rise,” says Dr. Susannah Baron, consultant dermatologist at Kent & Canterbury hospital, and BMI Chaucer Hospital. “Fragrance allergy can show up as contact dermatitis in the site a perfumed product is applied, or as a flare-up of existing eczema. It can be a real problem.” … Often it may not be immediately obvious that you’ve developed a fragrance allergy, says Dr. Baron. “You don’t react immediately; the body notes that it does not like the chemical and develops ‘memory cells,’ which cause inflammation when the body is next exposed to this chemical. Gradually, as you are exposed more and more, the body ramps up its reaction, until it becomes more noticeable to you.”
As the designer of the QEESI tool, Dr. Claudia Miller, an immunologist/allergist, explains based on her many years of research, that biological response is to the chemicals being used to produce the fragrances. Her pioneering work shows that exposures to chemicals of all kinds – not just the smelly ones – can and do trigger a loss of tolerance in some people, causing ill health.
And the simplest things can lead to new exposures, such as our recent utterly ridiculous adventures with installing a generator for our home. We often lose power, and so the prospect of Hurricane Sandy barreling down on us caused a run to the store and triggered a panicky purchase of a generator to help see us through.
Turned out we didn’t need to use it, and instead bought ourselves a world of trouble. In fact, what I didn’t know about it can be counted on all my fingers and toes in the dark, including the substantial extra costs of having an electrician hook it up properly, and the excruciating task of filling tanks up with gasoline, poised over the wafting fumes to ensure that I didn’t overfill the tanks and spill it all on my shoes.
To complete the misadventure, a small amount of gasoline did spill inside my car, rendering it nastily smelly once more. To get the odor out, I tried everything – wiping it down with baby oil, auto cleaners, and baking soda. Repeatedly.
Then I finally took it to a detail shop, and paid them a small fortune to use completely toxic cleaning supplies on the floor and seats. The smell has diminished, but it’s not gone, and it’s mingling with all the cleaners for a soupier feel. I still drive with the windows open and leave them all cracked while parked, at least when there’s no rain coming.
Contrary to what most folks think when they imagine what we are doing to “the environment,” indoor air is far more polluted than that outdoors. Given the number of people whose symptoms have been identified by the QEESI, I don’t think I’m alone in thinking that something is very wrong when the places we build – to live in, no less – are not particularly safe or comfortable for at least some living things.
So if you are like me, and these kinds of odors bother you as you go about your day-to-day, you may want to take the QEESI and see how and why they may be impacting you. And to learn what may be “masking” their effects, so that you don’t know where the headaches are coming from.
Even more pointedly, suppose you go on vacation and get a break from these exposures and feel suddenly better, which happened to a friend of mine, then you may want to start clearing your house of odoriferous chemicals and plastics to see if it makes a difference. It certainly did for her.
On the other hand, if you’re one of the lucky ones who feels just fine in this man-made world of olfactory offenders, well, then, you can snicker at us anti-chemical folk if you’d like to. But you may also want to think about whether those of us with the higher QEESI scores – and the concomitant fascination with “greening” our homes – are actually canaries in a mineshaft.
Tweet, tweet, I say, a bit sadly.
And because I’m a modern bird: Retweet? Are you a canary too?
October 29, 2012, 9:56 am
Dr. Nicholas Ashford, my co-author of the book Chemical Exposures: Low Levels and High Stakes, presented a thought-provoking analogy about how the same chemical exposure can affect people differently. His comments came at a National Academy of Sciences workshop in April 2012. I presented at the same workshop on TILT, or Toxicant-induced Loss of Tolerance; the QEESI, or Quick Environmental Exposure and Sensitivity Inventory; and the need for EMUs, or environmental medical units.
Here are Dr. Ashford’s remarks:
“Let me ask you to do a thought experiment. Suppose there were 10 Apple computers lined up along that front table and I were to open the motherboards of all those computers. Now suppose I were to take 10 pairs of those little Scottie magnets that your kids play with and I threw a pair of magnets into the motherboards of all 10 computers and then closed the computers and asked the first computer to add 2 and 2 and it gives me ‘minus 5.’ Then I asked the second computer how much is 2 and 2 and it says, ‘Well over 3.’ The third one just whirs. The fourth one doesn’t do anything, and so on, for each computer, down the line.
“Now if we had computer epidemiologists they would look at these 10 computers and they’d say they are all sick and each appears to have a different disease, i.e., each gives a different wrong answer to the question how much is 2 plus 2. If the epidemiologists didn’t see me throw the Scottie magnets into the computer, they would say these are unrelated diseases. Not only that, but the incidence of the malfunction — each rendition of a wrong, but different answer to the question how much is 2 plus 2 — would not be significant enough to say there was any disease in the population at all because not enough of the computers gave the same wrong answer. That’s what we’ve got with brain-mediated, brain-damage disease and I would argue that one of the bases for Toxicant-induced Loss of Tolerance is brain-mediated damage.
“When you throw a neurotoxic chemical into the brain, and you know a lot of them get into the brain, including the limbic system, which is where the immune system, the nervous system, and endocrine system converge, they may make the brain misbehave in a number of different ways. One of the ways in which it may misbehave may be endocrine disruption. Another way that it may misbehave is attention deficit hyperactivity disorder (ADHD). A third way in which it may misbehave is that autism can develop.
“Now I said it was a thought experiment, but probably the organ we know the least about and which is computer central to our entire existence is our brain. Toxicant-induced Loss of Tolerance can manifest in a number of seemingly unrelated ways, unexplained by classical toxicology that assumes a one-hit or single insult resulting in a single kind of pathology.”
Tags:
ADHD,
attention deficit hyperactivity disorder,
computers,
emus,
environmental medical units,
limbic,
magnets,
National Academy of Sciences,
neurotoxic,
QEESI,
Quick Envionmental Exposure and Sensitivity Inventory,
tilt,
toxicant-induced loss of tolerance Category:
Health |
Comment
August 20, 2012, 6:31 pm
No time of year brings more changes for children and teens than the start of a new school year. They return to different classrooms and often entirely new schools. Classrooms may have been remodeled, repainted, recarpeted, or treated with pesticides.
These changes can affect children regardless of grade level — pre-kindergarten, grade school, high school and college. Amid the back-to-school excitement, some students wind up feeling sick, listless or distracted, unlike last year. And parents wonder why, and what they can do. Sometimes the school environment is the cause.
Understanding why your child feels bad is especially challenging with children who cannot tell you what may be going on at school. What to do? How about visiting the school yourself?
I have a personal example: My son was returning to fifth grade and for the first time was struggling in math and other subjects. When I visited his school on parents’ night, I was struck by the strong odor of new rubber-backed carpet that had been glued down throughout the school. The classrooms formerly had wood floors and windows that opened to let in fresh air. The goal of the remodeling was to reduce noise. But my son and many other children and teachers became ill when they returned to school after summer break. The most subtle and common symptom was difficulty concentrating and remembering, but headaches, fatigue and worsening asthma also occurred — all as a result of well-intentioned remodeling over the summer!
How can parents detect the early signs of TILT, or Toxicant-induced Loss of Tolerance? TILT is a process that starts with a chemical exposure, such as in a “sick building,” after remodeling at school or home, or from cleaning chemicals or a pesticide exposure. It can cause susceptible individuals to lose their tolerance for everyday substances that never bothered them before, frequently including foods! Intolerances people develop are not usual “allergies.” See a detailed explanation of the differences.
Here’s a 7-point guide for recognizing the early signs of TILT:
- Over long weekends or during vacations away from school does your son or daughter feel better? Do they feel better just being outdoors? Pay particular attention to symptoms that occur when your child returns to school after a vacation. Do headaches, migraines, irritability, or other symptoms such as tics or stomach problems diminish when they are away from the school? Do the symptoms return “with a vengeance” once they return to classes? This is a useful “experiment”: avoiding the school for a week or so while on vacation, and then returning, paying close attention to symptoms. Re-exposure can evoke a “sharp response,” making it clearer which symptoms are related to a particular environment. Sometimes the return to school after the summer provides the clearest evidence — keep a symptom log on a wall calendar.
- Did your child’s health problem(s) begin with a flu-like illness and fatigue that did not go away?
- Does your child, and do other children from the school, report symptoms involving multiple organ systems, with a predominance of neurological symptoms such as fatigue, memory and concentration difficulties, sudden overwhelming sleepiness, headaches, confusion, unsteadiness/clumsiness, irritability or depression? But also, digestive difficulties, skin rashes, muscle weakness, sinus and nasal symptoms, recurrent infections, breathing problems (e.g. asthma) etc., that have become more frequent since school began. School nurses often have a handle on this and can be helpful if approached in a non-confrontational way.
-
Since your child returned to school, has she had any adverse or unusual reactions to medications, such as antihistamine/decongestants, antibiotics, antidepressants, injections, or general or local anesthetics (for example, at the dentist’s office)? This is particularly significant if the drug was formerly well-tolerated. It is an example of “loss of tolerance” due to exposure.
-
Does your child report feeling ill after meals, or that she is unable to tolerate foods she formerly enjoyed? Does your child have intense food cravings or feel ill if she misses a meal. Must she eat “on time” and or does she feel ill if a meal is missed? Does your child raid the refrigerator at night, e.g., for ice cream or other foods, drink large quantities of milk or sodas (corn sugar), eat chocolate or other candy, cookies, bread, popcorn/corn chips, or other foods “addictively.” Does she feel terrible the next morning from her food addictants?
-
Does your child use caffeine? What happens if she doesn’t get her usual amount each day? Is she now using increased amounts of caffeine or, alternatively, avoiding caffeine because it bothers her? Overuse and avoidance can both be signs of caffeine intolerance. Avoidance leads to withdrawal symptoms. As with drugs, overuse may help postpone/overcome caffeine and food withdrawal.
- Is your child hypersensitive to: 1) noise (crowds yelling at sports events, vacuum cleaner); 2) bright light (closes blinds, uses sunglasses indoors); 3) vibration/touch as when someone bumps into their bed; or 4) certain odors.
Be sure to notice when symptoms occur and whether any particular exposures/odors may have preceded them. For example, do felt-tip markers, engine exhaust, fragrances, odorous cleaning products such as bleach, nail polish/remover, hair spray, and phenolic disinfectants (those whose names end in “-sol”) now make your child feel ill or trigger symptoms? Use EPA’s “Tools for Schools” to work with your school district to choose the least toxic cleaning and pest control approaches, e.g., integrated pest management where least toxic approaches are used first. Another excellent resource is the Healthy Schools Network website.
My tip to parents: Record symptoms on a calendar, along with where your child was that day, foods they ate, and symptoms such as dark eye circles (so-called “raccoon eyes”), headaches, nasal stuffiness or runny nose, fatigue, stomach ache etc., rating symptom severity on a 0-10 scale, with “5″ being moderate symptoms and “10″ severe or disabling. Seizures would be “10.”
For more information and a validated, diagnostic questionnaire on TILT, see the Quick Environmental Exposure and Sensitivity Inventory, or QEESI, that can be downloaded without charge from my website. Fill it out, score it, and take it to your doctor along with your calendar/graph of symptoms over time.
Tags:
"raccoon eyes",
"sick building",
allergies,
asthma,
back to school,
Chemical intolerance,
cleaning chemicals,
fatigue,
migraines,
neurological symptoms,
pesticide exposure,
phenolic disinfectants,
school,
school rooms,
tilt,
toxicant-induced loss of tolerance Category:
Health |
Comment
July 20, 2012, 5:32 pm
Millions of dollars from the BP Claims Fund are being poured into healthcare efforts in the wake of the Deepwater Horizon disaster “to expand access to healthcare in underserved communities,” for “behavioral and mental health needs,” to “train community health care workers on peer listening, community resiliency and other related issues,” and to “expand and improve environmental health expertise, capacity and literacy.”
And yet, not one dime has been allocated to study how the toxic exposures resulting from this disaster have rendered thousands of workers and residents chemically sensitive and suffering from the same disabling multi-system symptoms that afflict the hundreds of thousands of American soldiers who suffer from what has become known as Gulf War Syndrome.
What we are witnessing, in fact, is the emergence of an entirely new disease mechanism that has grown out of the post-World War II petrochemical age and rendered millions of Americans who have suffered toxic exposures chronically ill. And the only way to help victims of toxic exposures and those in the future is to go after this mechanism.
How the settlement landed so far off the mark is anyone’s guess. One $14.4 million grant will send mental health counselors to the Gulf Coast.
People along the Gulf Coast are reacting to this news of misdirected largesse. As a reader of the Mobile (Ala.) Press-Register posted on the newspaper’s website, “Who will contain the money spill?”
Related link: My earlier message “To Gulf Oil Spill Responders: What You and Your Doctors Need to Know About TILT.”
Responders to the Deepwater Horizon spill, like the clean-up workers in the Exxon Valdez accident 20 years ago, have long been reporting chronic health problems associated with TILT, including multi-system symptoms (fatigue, sleep problems, headaches, digestive difficulties, and problems with memory and concentration) as well as new intolerances for everyday exposures that never bothered them before.
An article from the Huffington Post in March 2012 describes how doctors along the Gulf Coast are routinely treating clean-up workers and residents for chemical exposure and other problems that they blame on the spill. The article includes statements from a physician who uses the QEESI diagnostic questionnaire, Michael Robichaux, an otolaryngologist in Raceland, La., outside New Orleans.
Dr. Robichaux said he has treated 50 people for a range of health problems that he believes were caused by exposure to chemicals from the spill. “The illnesses are very real, and the people who are ill are apparently people who have sensitivities to these substances that not all of us are sensitive to,” he told the Huffington Post.
Patients suffering exposure symptoms may feel dizzy or nauseated around engine exhaust, cleaning chemicals, fragrances, or ill after meals, eating certain foods or even drinking one beer or glass of wine. These new intolerances are the hallmark symptom of a disease process called “TILT,” or “Toxicant-induced Loss of Tolerance.” We know that even so-called “safe” levels of exposure to toxic petroleum-based chemicals like those in the Gulf can initiate TILT. Once TILT develops, it is very difficult to treat, but TILT can be prevented.
To find out whether you may be susceptible to TILT or to track your symptoms, take the QEESI — a validated and published questionnaire I developed. You can download the QEESI at no charge under the “Publications & Presentations” tab.
July 19, 2012, 5:20 pm
Cases of childhood autism are up sharply, and there’s reason to wonder whether the number of cases is much higher than we suspect.
The Centers for Disease Control and Prevention reported in March that autism cases in the United States had increased 78 percent since 2002. That’s 1 in 88 U.S. children (1 in 54 boys and one in 252 girls), or about 1.1 percent of children.
A few weeks later, in May, a new study from South Korea reported that 2.3 percent of children there have autism. That’s twice the prevalence that the CDC has reported in the United States. Why such a difference?
The Korean study, lead by Yale and George Washington universities, counted cases differently. Researchers rigorously assessed individual children ages 7 to 12 in a community of 488,000 to identify known cases. In contrast, the CDC relied upon records of existing cases kept by health care and special education agencies.
Regardless of measuring methodologies, autism spectrum disorder now affects more children than diabetes, AIDS, cancer, cerebral palsy, cystic fibrosis, muscular dystrophy or Down syndrome – combined.
Why is autism on the rise? Better diagnosis alone can’t account for it.
The most cogent scientific explanation is also my greatest concern: chemical exposures. Chemically susceptible mothers who do not know they are susceptible and who therefore do not avoid exposures are at particular risk. They are more likely to have babies who share their susceptibility genes, and be raised in homes and environments in which exposures are relatively high compared to earlier generations. It’s a case where genetics loads the gun and the environment pulls the trigger.
Women who know they are chemically intolerant will work hard to help their families avoid things like pesticides, solvents, combustion products and other exposures that could lead to neurodevelopmental difficulties. This is because they are personally more aware of the adverse effects of these exposures. They will want to protect their children. However, women who are highly “masked” are less likely to avoid exposures. Although they may have multiple intolerances to foods, everyday chemicals and medications, they may be unable to tell which exposures are causing symptoms because triggering exposures occur throughout the day and their symptoms overlap in time.
The use of petroleum-based chemicals has risen dramatically in recent decades. These substances can seriously affect the health of susceptible people. With intense or long-term chemical exposures, these individuals can acquire Toxicant-induced Loss of Tolerance, or TILT. The problem is, currently, it is not always possible to know beforehand who is susceptible—before the parents build a new home or remodel their existing home for a new baby, hire an exterminator to keep bugs away and install air fresheners throughout the house so the home smells nice for baby.
New research suggests the children of chemically intolerant individuals inherit some of their parents’ same susceptibility to developing life-changing chemical, drug and food intolerances if sufficient exposure occurs (e.g., to pesticides, chemicals associated with new construction). The person develops TILT, or as some affected persons refer to the process, they become “TILTed.”
Most but not all chemical exposures are easy to identify by odor. Complex mixtures of chemicals emitted from everyday products used for home construction and furnishings, for example volatile organic chemicals outgassing from new carpet, adhesives, fragrances, etc., can be trapped inside our energy efficient, tightly constructed homes, schools and workplaces. These exposures can be hard to avoid and because of “olfactory adaptation,” our ability to smell complex low-level mixtures is quickly lost—within minutes of entering a home. Think of homes you may have visited while touring builders’ open houses: in your first few breaths you can smell the air, but after several breaths your nose adapts and you are no longer aware. A useful exercise can be to spend several days away from a suspect environment and then return, noting any odors that are apparent within the first breath or two. Or ask neighbors or friends what your house smells like — e.g ., mothballs, new carpet, a fragrance, natural gas or a mixture of substances?
Many of the same environmental exposures that initiate TILT can also interfere with neurodevelopment in a fetus. The harm can start as early as the first month of pregnancy. That’s the stage when the neural tube forms but before most mothers know they are is pregnant.
There are important relationships between autism, genes and exposures. Humans have different thresholds for becoming chemically susceptible. These differences are normal and not defects. These differences are not new. What is new? Our exposures.
Since World War II, the petrochemical era has ushered in countless new chemical exposures. Many of these have found their way into our building interiors where Americans spend on average 90 percent of their day. A mother and infant may spend even more time at home. Not only do indoor exposures vary from house to house and workplace to workplace, but there can be as much as a 10,000-fold difference between individuals in our ability to detoxify and eliminate certain substances from our bodies.
The rise in autism spectrum disorders seems to follow the rise in petrochemical usage, and arouses enough suspicion to justify immediate research.
The need for research is great, and future studies need to focus on potential environmental causes and especially the indoor environment—an area that falls between the cracks in terms of government research funding. There is a saying: “There are no genetic epidemics.” If a condition has become as prevalent as autism, then research must examine potential environmental contributors — and quickly. Although genes play a role in terms of individual susceptibility to exposures, it is the exposures that are the problem, not our genes! In March, Mark Roithmayr, president of the influential organization Autism Speaks, which helped fund the South Korean study, called for a comprehensive national strategy to address the autism epidemic. Among other things, he cited a need to:
- Fund more basic science uncovering the genetic underpinnings of autism.
- Fund more environmental research detecting the causes of autism.
- Accelerate the funding and development of effective medicines and treatments.
I agree with his statement. There are many different types of autism. Autism is an umbrella diagnosis, one that has many potential root causes. However, the “chemical connection” seems be one of the most promising paths toward an understanding of autism spectrum disorder.
July 10, 2012, 2:42 pm
Chemical intolerance contributes to the illnesses of 1 in 5 patients but the condition seldom figures in their diagnosis, according to clinical research published July 9 in the journal Annals of Family Medicine.
(Note: I was a co-author of the paper, which is available from the Annals of Family Medicine website. The study struck a national nerve, and it has been reported widely in the news media, including highly-read Medscape.com, which ran an excellent account. You’ll need a free Medscape login and password to view it. Other accounts are published at Science Daily and Fox News.)
Here’s a summary sent to the media:
Chemical intolerance contributes to the illnesses of 1 in 5 patients but the condition seldom figures in their diagnosis, according to clinical research published July 9 in the journal Annals of Family Medicine.
Clinical tools are available to identify chemical intolerance but health care practitioners may not be using them, said lead author Dr. David Katerndahl, professor of family and community medicine at the University of Texas Health Science Center at San Antonio.
The study’s authors said physicians need to know how chemical intolerance affects certain people and understand that conventional therapies can be ineffective. Some patients would improve by avoiding certain chemicals, foods and even medical prescriptions, the authors said.
Patients with chemical intolerance go to the doctor more than others, are prone to having multi-system symptoms and are more apt to have to quit their job due to physical impairment, the authors said.
The study involved 400 patients who gave personal health information while waiting to be seen at primary care clinics in San Antonio. The researchers asked the patients to respond to 90 questions about their illnesses, mental health and ability to function.
In the end, the authors said, 20.3 percent of the patients questioned met the scientific criteria for chemical intolerance.
Researchers surveyed patients with chronic conditions such as allergies, asthma, diabetes and heart disease. They excluded patients who were at the clinics for acute conditions such as earaches, flu or bone fractures.
The origins of chemical intolerance have been the subject of much speculation, the authors acknowledge, but the condition is also understudied. People with chemical intolerance, or “CI,” are highly sensitive to common substances such as cleaning products, tobacco smoke, fragrances, pesticides, new carpet and auto exhaust.
“Apart from the debate over causality, the fact that so many patients meet the criteria for chemical intolerance holds particular relevance for primary care providers,” said Dr. Katerndahl.
Chemically intolerant individuals often have symptoms that affect multiple organ systems simultaneously, especially the nervous system. Symptoms commonly include fatigue, changes in mood, difficulty thinking and digestive problems.
Study co-authors are Dr. Claudia S. Miller, professor in environmental and occupational medicine, vice chair of family and community medicine, and director of the South Texas Environmental Education and Research (STEER) Program, among her roles; Dr. Raymond F. Palmer, associate professor of family and community medicine at the University of Texas Health Science Center at San Antonio; and Dr. Iris R. Bell, professor emeritus in the Department of Family and Community Medicine at the University of Arizona College of Medicine and research professor in the College of Nursing at the University of Arizona.
An added comment: Healthcare professionals as well as the public can assess chemical, food, drug and other intolerances using the QEESI, the Quick Environmental Exposure and Sensitivity Inventory, which I developed. It is available free for download.
Tags:
auto exhaust,
Chemical intolerance,
cleaning products,
digestive problems,
fatigue,
fragrances,
mood,
new carpet,
pesticides,
thinking problems,
tobacco smoke Category:
Research |
Comment
June 12, 2012, 4:59 pm
I presented April 18 at the National Academy of Sciences Workshop “Biological Factors that Underlie Individual Susceptibility to Environmental Stressors and Their Implications for Decision-Making.”
The proceedings are available by recorded webcast so you can view and listen to the speakers. View the webcast at:
http://www.tvworldwide.com/events/nrc/120418/
(Supply your email adress to log in.)
The title of my presentation was “Human Variability in Chemical Susceptibility (Intolerance/Sensitivity): Research Findings to Date and Their Implications for Future Study Design.” I’ve posted my presentation for your review.
I was asked to describe our findings from the QEESI, the Quick Environmental Exposure and Sensitivity Inventory, and to discuss the use of EMUs, environmentally-controlled medical units, for research. Here is a synopsis:
“The QEESI is a validated research tool widely used to identify and characterize chemically intolerant individuals and groups. Results from these studies provide evidence for broad endogenous variability in susceptibility and point to the complex nature of susceptibility in humans, with susceptible persons generally reporting adverse responses to chemically diverse substances, including foods and drugs. Future investigations to assess human variability that is ‘endogenous or biological’ will benefit from the use of EMUs. Such studies will enable us to correlate symptoms and clinical measures (such as pulmonary function and EEG measures) with changes in the ‘-omics’ in real time at key points, i.e., when subjects enter the EMU, once they have achieved a clean baseline, and pre- and post- low level challenges.”
The QEESI is available free for download.
Details about the workshop are at:
http://nas-sites.org/emergingscience/workshops/individual-variability/
Tags:
chemical,
Chemical intolerance,
chemical sensitivity,
drug intolerance,
drug sensitivity,
emerging science,
emu,
emus,
endogenous factors,
environmental medical unit,
environmental stressors,
environmentally controlled medical unit,
food intolerance,
food sensitivity,
genomics,
individual differences,
individual susceptibility,
individual variability,
intolerance,
low level exposure,
multiple chemical sensitivity,
nas,
National Academy of Sciences,
QEESI,
sensitivity,
stressors,
susceptibility Category:
Research |
Comment
May 8, 2012, 5:32 pm
The Pulitzer Prize-winning publication ProPublica drew attention in May to the lack of centralized data on implanted medical devices. Where can patients find out when a pacemaker, breast implant or artificial hip, for example, goes bad?
Not from the U.S. Food and Drug Administration, as ProPublica’s story describes. Prescription drugs have unique codes the government can use to track problems. But implanted devices? No such luck.
And there’s an unexplored dimension to the implant question: Implants are “xenobiotics,” petrochemical products that pose particular concern for people who may be more chemically susceptible.
I testified before the FDA in 2005 about the dangers of implants, and cited evidence from my own research.
Over a decade ago, in 1999, along with co-author Thomas J. Prihoda, PhD, I reported on a group of patients who received implants and subsequently developed chronic health problems and chemical intolerances that they had never experienced before.
Although inserting implants certainly differs from inhaled exposures to pesticides or air contaminants in a sick building, for susceptible individuals it seems like the body doesn’t care whether the exposure is exogenous (like air pollutants) or endogenous, like an implant. The consequences can be similar — chronic, multi-system symptoms and intolerances for foods, alcoholic beverages, caffeine, everyday chemicals like cleaning agents, engine exhaust, fragrances, and even medications like antibiotics or antidepressants. Once people become ill, not just the implants, but everyday exposures like these can trigger symptoms and perpetuate illness.
We obtained exposure histories from patients who became ill following an “exposure event” — ill veterans from the first Gulf War in Iraq, people exposed to pesticides or remodeling chemicals, and patients who had received an implanted medical device. The groups shared illnesses marked by multiple symptoms and new intolerances — the hallmark symptom of the illness process Toxicant-induced Loss of Tolerance (TILT).
Patients with implants reported symptoms affecting multiple organ systems which frequently involved cognitive and mood difficulties.
The implant group included 87 individuals, 97 percent women, mean age of 50. Most had received breast implants or temporomandibular joint (TMJ or jaw) implants. Two-thirds said their device had ruptured. Nearly all of those reporting difficulties said their illnesses had affected their ability to work. Their most pervasive symptoms involved muscle and joint problems.
TILT is often overlooked in implant patients when doctors don’t recognize it. There is a saying in medicine: You can’t make the diagnosis you don’t think of. And many doctors don’t know that multiple symptoms and intolerances point to TILT. In medical school, we are often taught that the more symptoms a patient reports, the less likely there is anything to them — in other words, the problem is psychogenic. While many patients suffer from psychological symptoms such as depression, anxiety and cognitive difficulties, even confusion, it is important to remember that psychological symptoms are not necessarily psychogenic. Many physical illnesses can cause similar symptoms, for example, autoimmune diseases, multiple sclerosis and Lou Gehrig’s disease (ALS).
As I wrote in the 1999 study, “The fact patients reported such diverse symptoms led some physicians to conclude that none of them rises to the level of a medically identifiable syndrome. Nor are these conditions explained by current, generally accepted mechanisms for disease.”
I developed the QEESI, or Quick Environmental Exposure and Sensitivity Inventory, several years ago to help doctors and patients make sense of multiple symptoms and measure the potential for chemical intolerance.
Persons who score high on the QEESI, a validated and published screening instrument, may be at greater risk if they receive an implant or have other exposures, e.g., anesthetics, drugs, pesticides, remodeling of their home or workplace, etc. To determine whether you may be at increased risk of developing TILT, you can take the QEESI to gauge your own susceptibility or to document changes in your symptoms and intolerances as a consequence of an implant or its removal. Many individuals do report improvement in symptoms once their implants are removed.
As for the FDA, the regulatory agency has done poorly in its role of gathering scientific data about the safety of implants. Dr. Diana Zuckerman, president of the National Research Center for Women and Families, a research and education group, told an expert panel of the FDA in 2011 that some breast implant manufacturers had failed to carry out the FDA’s own recommended studies of post-implant patients. One of the FDA’s chief scientists, Dr. William Maisel, later acknowledged shortcomings when questioned by the New York Times.
Commenting on breast implants in her blog, Dr. Zuckerman added, “Silicone implants are considered biocompatible, which means that most patients won’t have an allergic or autoimmune response. But, that doesn’t mean that nobody will. In fact, the implant companies intentionally excluded women with autoimmune histories from their studies because of concern that the women would have medical complications that would jeopardize getting FDA approval.”
When I’ve testified before the FDA on the results of our study, I’ve been concerned with the fact that parents may purchase implants for their daughters for their “Sweet 16” or high school graduation. Adverse events include scarring as well as chemical intolerances in a subset of individuals. The problem is, that before an implant, there is currently no way of knowing who may be more susceptible to developing health problems or disfigurement. The QEESI might at least make women more aware if they are susceptible to petrochemical exposures, including implants. I’ve heard of women who already had been diagnosed with an autoimmune disease going to see a doctor to get implants. No doctor should agree to place breasts implants in women with this history.
Also, I’m aware of young women borrowing money to get an implant. However, if they become ill, insurers may not pay to have them removed. So it’s not just the cost of the implant, but the unplanned costs if removal becomes necessary.
Tags:
breast,
breast implant,
chemical exposure,
Chemical intolerance,
implant,
multi-system symptoms,
QEESI,
silicone,
sweet 16,
tilt,
tmj,
toxicant-induced loss of tolerance,
xenobiotics Category:
Research |
Comment
March 20, 2012, 9:52 am
Is there a way to make “green” buildings as friendly to people as they are to the environment?
I had the opportunity to discuss indoor air quality and chemical susceptibility with some of the nation’s leading architects and building technologists at a recent conference about building standards. I was one of 13 guest speakers at the conference hosted by the School of Architecture at the University of Texas in Austin.
Indoor air has a profound effect on people’s health, and my goal was to persuade the group that poor quality air makes some people sick. My message was simple: If you protect the most vulnerable people, you will protect everyone.
I suggested adding a new level to the coveted LEED building certification. The new certification level would recognize buildings that assure excellent indoor air quality.
Certification under LEED, short for “Leadership in Energy and Environmental Design,” reflects a rating system for the design, construction and operation of green buildings. Developed by the U.S. Green Building Council, it is intended to provide building owners and operators with a framework for identifying and implementing practical and measurable green building design, construction, operations and maintenance solutions. Buildings receive LEED certification based on five categories of construction quality. I proposed a sixth: indoor air quality. A building can be LEED certified and yet have indoor air exposures that pose major health problems for a building’s most susceptible occupants, such as the chemically intolerant, those with asthma, pregnant women, etc.
Americans spend 90 percent of their day indoors so architects and builders bear a major responsibility for the quality of indoor air.
Who is most vulnerable? Children, pregnant women, and more susceptible adults (people with asthma, allergies, or chemical intolerance). At any given time, of 100 people, 3 are pregnant or will become pregnant within a year, 7 are children under the age of 5 (another 17 are still under the age of 18 and the brain continues to develop into the early 20s!), 7 have asthma, 20 have
allergies, and 15 are chemically intolerant.
LEED certification does not protect the most vulnerable building occupants from indoor air contaminants such as chemicals, particles, allergens, and microbes. Although indoor environmental quality requirements are part of LEED certification and builders and owners can earn points by taking additional measures that can improve indoor air quality, the levels of certification such as “silver,”"gold,” or “platinum” are insufficient to protect the most vulnerable building occupants. A new designation, perhaps “LEED Diamond,” should be introduced with mandatory criteria to ensure excellent indoor air and protect all building occupants.
My presentation is available in .pdf and PowerPoint.
February 17, 2012, 6:06 pm
Scientists, healthcare professionals and especially people with chemical intolerance have achieved a victory that took years to win. In a nutshell: High-level U.S. policymakers now say chemical intolerance needs serious investigation.
The recently concluded “National Conversation on Public Health and Chemical Exposures,” sponsored by several government agencies, issued a detailed statement in October 2011 that summed up two years of deliberation among hundreds of experts. The statement, in brief, calls for intensified work to understand chemicals and their health effects.
I think the statement will influence health policy and promote new research and clinical inquiry. Progress in the science, diagnosis and treatment of chemically-induced illness has been painfully slow. I’m excited to see this new development.
The National Conversation, in its final statement, urged intensified study of:
- Health effects of chemicals, including low-dose, multiple and cumulative exposures
- Individual susceptibility, including the interplay between genes and environment
- Community vulnerability and disproportionate effects from past exposures
- Effectiveness of interventions to protect public health
To me, one of the most important recommendations called for human studies using environmentally controlled research units. It said: “Studies of variation in susceptibility as manifested by chemical sensitivity/intolerance, including clinical studies conducted in facilities adequate for this purpose, are needed.”
This recommendation for research facilities first appeared in a report commissioned by the State of New Jersey that I co-authored in 1989 with Nicholas A. Ashford, Ph.D., J.D., professor at Massachusetts Institute of Technology, as well as in subsequent editions of our book Chemical Exposures: Low Levels and High Stakes.
Here is an excerpt from recommendations in the National Conversation’s report “Chapter 3: Achieve a More Complete Scientific Understanding of Chemicals and Their Health Effects”:
“Recommendation 3.5: Improve understanding of individual susceptibility to chemical exposures.”
“Those seeking to protect the public from the adverse effects of chemical exposures need a better understanding of variations in individual susceptibility to help prioritize prevention and treatment efforts. Some individuals in certain groups (e.g., developing fetuses, children, pregnant women, the elderly, disabled persons, persons with chronic diseases, persons with previous heightened sensitivity to chemical exposures) exhibit unique susceptibility to chemical exposures. Some of this variability in susceptibility may be related to genetic variation, acquired epigenetic changes, health effects from previous exposures, or nonchemical stressors. To improve the understanding of these variations, funding agencies should continue to support research into mechanisms of variation in individual susceptibility and the role of such variations in the observed burden of environmentally related disease. Studies of variation in susceptibility as manifested by chemical sensitivity/intolerance, including clinical studies conducted in facilities adequate for this purpose, are needed. Population-based studies of exposed groups may yield additional insights.”
“Further, the federal government should support an existing working group or convene an interdisciplinary group of scientists and clinicians from federal agencies, NGOs/public interest groups, industry, academic institutions, and representatives of affected patient communities to develop a research agenda on chemical sensitivity/intolerance.”
The National Conversation was a two-year collaborative process that produced an action agenda in June 2011 on new ways to protect the public from harmful chemical exposures. In October 2011, the leadership issued its final recommendations at an implementation strategy session in Washington, D.C., hosted by the American Public Health Association (APHA).
I chaired the National Conversation’s subgroup on Individual Susceptibility, and served as a member of the larger Scientific Understanding Work Group, one of six working groups assigned to various aspects of chemical exposure. The work group issued a full-text action agenda.
As part of their mission to advance the public’s health, the Centers for Disease Control and Prevention and the Agency for Toxic Substances and Disease Registry supported the National Conversation. Dozens of government agency, nonprofit and industry experts and thousands of members of the public were involved in developing the recommendations.
Tags:
chemical,
chemical exposures,
Chemical intolerance,
cumulative exposures,
environmental,
environmentally controlled environmental unit,
epigenetic,
exposure,
low dose,
low level,
medical unit,
multiple exposures,
national conversation,
sensitivity,
susceptibility,
tilt Category:
Research |
Comment
January 27, 2012, 7:43 pm
Flight delays, missed connections, stuffy cabins, narrow seats, screaming children. As if commercial air travel isn’t hard enough, now comes evidence that it could be harmful to your health.
In recent lawsuits and public complaints, dozens of passengers and airline personnel report inflight chemical exposures that triggered serious illnesses. The illnesses are similar to those associated with “Toxicant-induced Lack of Tolerance,” or TILT, a clinical condition that breaks down a person’s natural resistance to chemical compounds.
The Boeing Co. recently settled a suit out of court in Seattle with a former American Airlines flight attendant. She alleged that contaminated cabin air in an MD-82 jetliner caused her to have tremors, memory loss and severe headaches. US Airways pilots and flight attendants have filed a similar suit involving a Boeing 767. They reported headaches, sore throats, eye irritations, dizziness and nausea.
A similar incident in 2011 involving a Lufthansa Airlines jumbo jet came to light in December 2013. The trade publication Aviation Herald said the crew aboard the Airbus A380 detected a “chemical odor of dirty socks” when the plane took off from Frankfurt en route to San Francisco.
One flight attendant reported feeling ill after the incident and has been unable to return to work due to headaches, fatigue, poor concentration and eye irritation, the publication said. Subsequent lab tests on the flight attendant identified exposure to the neurotoxin tricresyl phosphate, an organophosphate used in aviation lubricants, the publication said.
At issue are so-called “fume events” where petroleum smells enter the aircraft cabin. Commercial airliners routinely pump, or “bleed,” compressed air to the cabin from outside. Nearly all airliners use this “bleed-air” ventilation system. The airline industry and government regulators say the system is safe, and has been in use since the 1950s. The industry says the number of reports of illness is minuscule compared to the thousands of people who fly each day.
Critics say bleed-air systems draw a substantial amount of air past the engine, thus raising the risk that petroleum fumes can enter the cabin. Loose engine seals and poor aircraft maintenance raise the chances that air can become contaminated on its way to the cabin.
Air travel is difficult for people with chemical intolerances, but until recently no one suspected that taking a flight might trigger illnesses in otherwise healthy people. Finding solutions is urgent because the sheer volume of passenger traffic may leave hundreds of thousands of people exposed and vulnerable to a new sickness.
On any plane, the people most affected by a lack of fresh air usually have asthma, suffer migraines, or are already chemically intolerant. It’s fortunate that the largest amount of fresh air is sent to the flight deck, where the pilot and co-pilot fly the plane. But even pilots and co-pilots have reported illnesses and, in a few cases, even impaired cognitive function.
Even under normal conditions, an air traveler’s “breathing zone” is frequently violated on flights. Some examples:
- Boarding the plane, passengers sometimes enter a hot plane with little fresh air. Some of them get headaches or have difficulty breathing. Crews often turn off the PAC, or air-conditioning system, to save fuel. My advice: Ask the crew to turn it on.
- Once seated, passengers encounter unpleasant odors — from perhaps from a cigar smoker seated nearby, those wearing fragrances, or others using nail polish. Again, as a passenger, your breathing zone is violated, and you’re stuck for the duration of the flight.
- Waiting for takeoff, passengers sometimes breathe exhaust from other planes lined up ahead of them.
- Also, the fragrance from restroom deodorizers can cause problems. I was on a recent flight and the odor was intense. Putting potent deodorizers in tiny spaces can cause a very high concentration of fragrance. Passengers also carry the fragrance back to their seat. Recommendation: Sit in the middle of the plane. That way fewer passengers will drag their restroom fragrance vapor trails past your aisle.
Facts and narratives about airplane illnesses are becoming more widely known. MSNBC.com reporter Jim Gold has written an excellent article about the situation.
Passengers may have few defenses, but scientists are working to minimize exposures aboard airplanes. In his article, Gold describes efforts to develop a biomarker for TCPs, or tricresyl phosphates, one of the suspected contaminants in fume events. One key researcher, Dr. Clement Furlong of the University of Washington, said the goal is to better understand the chemistry of the incidents so refiners can develop less-toxic engine fluids. This might improve the bleed-air system, or at least minimize its potential risks to health.
TCP is the cause of numerous poisonings and is a neurotoxin, in part via organophosphate-induced delayed neuropathy. It has been responsible for many deaths. The most serious incidents occurred in the 1920s when TCP was used to adulterate Jamaica Ginger, and in Morocco in 1959 when cooking oil was adulterated with jet-engine lubricant containing TCP.
TCP’s mechanism of action is similar to other organophosphates in that it can inhibit the enzyme acetylcholinesterase, leading to a buildup of acetylcholine in the synaptic space. This can lead to hyperactivity in cholinergic neurons in the brain, and at neuromuscular junctions in the peripheral nervous system resulting in apoptosis of those cell types. This is the reason for paralysis and other irreversible neurological problems seen in the “Gingerjake” syndromes during Prohibition, when TCP was added to gingerjake moonshine.
Dr. Furlong is working to develop a blood test to prove with a biomarker that someone aboard an aircraft during a fume event was exposed to TCPs. A reliable test would dispel the uncertainty now in the air for air travelers.
TCP is one of many substances capable of initiating TILT. However chlorpyrifos, or Dursban, is one of the most common causes. Why has chlorpyrifos initiated so many illnesses? You may want to review a paper I co-authored in the Archives of Environmental Health about initiators. Note mention of TCP on page 121.
Symptoms and health effects of TILT often accumulate over time. People can gauge their sensitivities using the free QEESI questionnaire. It is a clinical tool to evaluate whether someone has TILT or is acquiring intolerances.
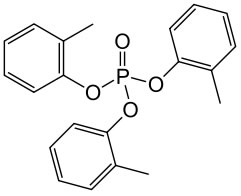
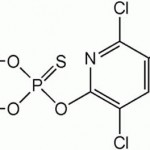
Illustrations depict chemical structures of TCP, left, and chlorpyrifos, or Dursban, which is one of the most commonly reported initiators of TILT.
October 23, 2011, 12:49 pm
Medical researchers are finding that children with autism and their parents suffer in some of the same ways when they encounter certain chemicals in everyday products.
Recently, at the invitation of the Autism Society of America, I presented a national webinar describing how children with autism and their parents often share certain intolerances, and may react in similar ways. Why? I think it’s a case where “Genetics loads the gun, and the environment pulls the trigger.”
We know, for example, that in adults certain acute or chronic chemical exposures sometimes can initiate a process that has come to be known as “Toxicant-induced Loss of Tolerance,” or TILT. TILT may develop after a workplace exposure or remodeling of a home or exposure to petrochemicals or combustion products from a fire. Thereafter, everyday exposures to common chemicals, foods, medications, and even caffeine, can trigger cognitive and mood difficulties, as well as a host of baffling symptoms that can affect the nervous system, digestive tract, airways, and skin.
Notably, many of the same environmental exposures, e.g., certain pesticides, that initiate TILT in adults can also interfere with neurodevelopment in a fetus, starting as early as the first month of pregnancy when the neural tube forms and before the mother even knows she is pregnant!
And, as for chemically intolerant adults, we should make every effort to prevent suspected initiating exposures as well as minimize exposures that can continue to trigger autistic behaviors and other symptoms throughout the lifespan. This also means that continued avoidance of even low-level exposure triggers may be important for treating children and adults with autism.
These differences in susceptibility to environmental chemical exposures, which may predispose to TILT in adults and autism in children, are the consequence of normal human genetic diversity — a good thing! My concern, as we learn more about the important relationships between autism, genes and exposures, is that differences in our genetic susceptibility not be viewed as a defects, but rather normal individual differences. These differences are not new. What is new are our exposures. Since World War II, the petrochemical era has ushered in myriad chemical exposures, exposures unprecedented in human history. There can be as much as a 10,000-fold difference, from person to person, in our ability to detoxify and eliminate substances from our bodies. Currently we are unable predict which exposures can cause TILT or autism in which persons.
Other shared features of autism and chemical intolerance include food cravings (mimicking addiction) and intolerances including gluten (wheat) and milk. From our own studies, mothers of children with autism, compared to mothers of “neurotypical children’” were much more likely to report that common chemical exposures make them sick. These included household cleaners, fragrances and pesticides. We used the validated “Quick Environmental Exposure and Sensitivity Inventory” or QEESI, questionnaire to gauge chemical, food and other environmental intolerances in the mothers. You too can use the QEESI questionnaire to gauge sensitivities.
The underlying causes for autism and the reasons why it now affects a staggering 1 in 110 babies born in the United States — a national epidemic according to the Centers for Disease Control and Prevention (CDC) — continue to elude the medical and scientific communities. There are many clues, and theories. The webinar I presented on behalf of the Autism Society of America, which is available to you free of charge, focuses on the striking and often overlooked parallels between autism and chemical intolerance. The increased use of petrochemically based household products and recent emphasis on greener, more energy efficient homes with little fresh air to dilute contaminants in the United States parallels the rise in autism over the past few decades. Globally, autism has been on the rise in every industrialized nation.
During medical school, my colleagues and I learned that children are not just little adults! There are obvious size and many metabolic differences between children and adults. At the same time, children with autism and chemically intolerant adults are strikingly similar in important ways: They share exposures to petrochemicals, indoor air pollutants and pesticides, and both experience chemical and food intolerances. A crucial difference in the case of autism is timing: Exposures that occur during pregnancy or early childhood have the potential to alter neurodevelopment. One tool that is urgently needed in medicine is an Environmental Medical Unit, or EMU, which would allow physicians and families to determine whether and to what extent autism might be reversible if chemical and food triggers could be avoided systematically for a few weeks. Here is a paper I wrote about EMUs.
Here is the webinar presentation to the Autism Society of America.
To follow the proceedings, you will need to install the Cisco Webex browser software. You will be prompted at the website. Adding the software only takes a few seconds.
Tags:
ASA,
ASD,
Autism,
Autism Society of America,
autism spectrum disorder,
Chemical intolerance,
chemical sensitivity (hidden tag),
fragrance,
indoor air,
pesticide,
QEESI,
tilt Category:
Autism |
Comment
November 17, 2010, 3:14 pm
Fragrances are among the most frequent and potent symptom triggers for people who report developing chemical intolerances following an acute or chronic exposure such as to pesticides or indoor air pollutants. Sometimes specific formulations (air fresheners, fabric softeners, etc.) or brands are especially problematic, with individuals reporting headaches, impaired concentration, confusion, sudden mood changes, fatigue, etc.
Anne Steinemann at the University of Washington and her colleagues recently analyzed 25 top-selling fragranced consumer products. The paper, which can be accessed here, is an eye-opener. Using GC/MS (gas chromatography/mass spectrometry), Steinemann found that these products contain an average of 17 chemicals each, almost all of which do not appear on any label, and many of which are known to be toxic. A single fragrance may contain 100 or more VOCs. This strongly suggests that we need to find unscented alternatives for cleaning our homes, our laundry and ourselves.
Q: Why don’t the names of these chemicals at least appear on the product labels? A: Manufacturers are not required to disclose fragrances in cleaning supplies, air fresheners or laundry products. These are regulated by the Consumer Product Safety Commission. Likewise, the Food and Drug Administration, which regulates personal care products, does not require listing of ingredients used in fragrances, “even though a single “fragrance” in a product can be a mixture of up to several hundred ingredients.” Ms. Emily Sohn, writer for Discovery News, asked me to comment on the significance of this new study. Read the article here.
As an allergist, I know that individuals’ responses to exposures vary widely. The problem is, we can’t know a priori whether or in whom a scent is going to cause nasal congestion, a headache or impair the ability to concentrate-at home, at work, at school or while driving. We do know that a sizable percentage of the population responds adversely to various fragrances and other low-level exposures.
Fortunately, there is something we can do. We can stop buying fragranced products, instead choosing those that are clearly labeled “fragrance-free.” Tell the managers at places you and your family frequent, from the grocery store to restaurants to your child’s school, that you want fragrance-free products used because of the hazardous chemicals found in many fragranced products. There is no way to know how toxic a specific fragranced product may actually be, and as Steinemann found, simply choosing products that are “green” or “natural” is no guarantee of their safety. Fragranced “green” products, she reported, also emitted volatile organic compounds (VOCs) which can irritate the airways and cause multi-system symptoms in susceptible individuals.
Individuals with chemical intolerances can benefit greatly from fragrance-free policies at school or work and from eliminating fragrances at home. Unfortunately, while fragrance-free policies can help protect building occupants and custodial staff from harmful chemicals, one of the greatest sources of fragrances indoors is other people. Many people start off their day by applying a variety of fragranced products, which then volatilize into the air throughout the day. This personal “out-gassing” is worst in the morning, and it can be debilitating for chemically intolerant individuals if they must start their day sitting next to someone at a meeting or in class, inhaling complex mixtures from fabric softeners, personal care products, and cologne.
Fragrance intolerance may be an important sentinel symptom for Toxicant-induced Loss of Tolerance (TILT). There is a close anatomical relationship between the nose and the limbic (mood and memory) part of the brain. People tend to notice when a fragrance that was once loved now makes them feel ill. In my work with Gulf War I veterans, I met a soldier who sent his spouse their favorite fragrance while still he was overseas. After he returned from Iraq, she went to pick him up from the airport wearing that special scent. During the several-hour drive back home, he became so sick that he begged her never to wear it again.
I firmly believe that “Your right to wear fragrance ends at my nose,” a phrase adapted from the days when smoking indoors was still common. But, regardless of who is right, the best strategy when seated next to a heavily fragranced person is to move. It is tiresome to feel you are “on the run,” from invisible vapors of fragrance, but as more people gently explain that fragrance causes headaches, asthma, burning eyes, or nausea, perhaps both policies and personal choices will change.
One woman I know has recently been trying a new approach. When she sits next to individuals who aren’t wearing discernible fragrances, she thanks them, saying, “I want to thank you for not wearing fragrance. I often have to get up and move because other people’s perfume and laundry products can give me a headache.”
It’s a great conversation starter.
Remember: Fresh air is the best air freshener, and the best smell is no smell!
September 22, 2010, 6:54 am
Sunday, September 12, 2010
Newswise — Swimming in indoor chlorinated pools may induce genotoxicity (DNA damage that may lead to cancer) as well as respiratory effects, but the positive health effects of swimming can be maintained by reducing pool levels of the chemicals behind these potential health risks, according to a new study published in a set of three articles online September 12 ahead of print in the peer-reviewed journal Environmental Health Perspectives (EHP). This study is the first to provide a comprehensive characterization of disinfection by-products (DBPs) in an indoor pool environment and the first to study the genotoxicity of exposure to these chemicals among swimmers in an indoor chlorinated pool.
DBPs form in pool water from reactions between disinfectants such as chlorine and organic matter that is either present naturally or is introduced by swimmers, such as sweat, skin cells, and urine. Previous epidemiologic studies have found an association between exposure to DBPs in drinking water and risk of bladder cancer, and one such study has found this association for dermal/inhalational exposure such as occurs during showering, bathing, or swimming.
Chemicals in Indoor Swimming Pools May Increase Cancer Risk
May 26, 2010, 12:15 pm
Share your story of chemical exposure and loss of tolerance by responding to this post. If we feel your story may be helpful to others learning about TILT, Dr. Miller will re-post your story with her comments. Be aware that you are posting your story in a public forum. Do not include identifying information unless you are comfortable with it being available to anyone on the web, and please do not post your story if you are pursing any legal action regarding your exposure or TILT-related illness. We also ask that you do not name any third parties including doctors, coworkers or family members. We will remove any postings that are not appropriate to this forum and the topics we address.
Following is a format you may wish to follow in describing your experiences. Specific information is most helpful.
Initiating exposure(s): What was it? Which year did it occur?
How many others were exposed and did they develop TILT?
Fill out the QEESI – what are your scores on the 5 scales, both now and when you were at your worst?
After the initial exposure, how soon did your intolerances begin? Which did you notice first? Which caused the most severe symptoms?
Please indicate if you have experienced the following types of intolerance, and describe your principal reactions/symptoms.
Chemical intolerances:
Food intolerances:
Caffeine intolerance:
Alcoholic beverage intolerance:
Adverse drug reactions or drug intolerance:
What medical diagnoses have you or other affected family members received since developing TILT?
How many doctors did you see before you figured out what had happened to you?